Clinical Analysis and Red Flag Signs in Pediatric Headache According to Age
Article information

Abstract
Purpose
The clinical characteristics of headaches vary by age among pediatric patients. Red flag signs are key factors in differentiating secondary headaches and should be considered in the context of the patient’s age.
Methods
This study involved a retrospective chart review of pediatric patients presenting with headaches. Patients were categorized by age into three groups: pre-school age (under 6 years), school-age (6 to 12 years), and adolescence (over 12 years). Demographic data, headache characteristics, laboratory findings, and neuroimaging results were evaluated. Overall, 17 potential red flags were assessed.
Results
A total of 687 patients were included, of whom 102 were of pre-school age, 314 were school-aged, and 271 were adolescents. The frequency of overweight/obesity was found to increase with age. The pre-school age group experienced a shorter period from symptom onset to presentation and a briefer duration of pain. In contrast, adolescents displayed a longer period from symptom onset, a greater frequency of headaches occurring at least three times per week, and a higher rate of headache episodes lasting over 3 days. Children under 6 years old were more commonly diagnosed with secondary headaches than older children. Across age groups, secondary headaches were suspected when systemic symptoms such as fever were present, when the headache had a sudden onset, when the patient responded poorly to medication, or when abnormal neurological signs and symptoms were observed.
Conclusion
The clinical features of pediatric patients vary by age group. Clinicians should consider red flag signs in the context of patient age and individual characteristics.
Introduction
Headaches are among the most common reasons for admission to pediatric neurology clinics. The reported prevalence of headaches among children ranges from 37.0% to 51.0% [1]. While comparatively rare among younger children, this symptom warrants increased attention and necessitates a distinct diagnostic approach due to the high risk of secondary headaches [2]. In addition, younger children often struggle to articulate their symptoms and may exhibit vomiting, irritability, or behavioral changes rather than the typical patterns associated with primary headaches. This complicates the diagnostic process and necessitates extensive workup [2]. In contrast, the incidence of headaches tends to rise throughout adolescence. Although adolescents generally exhibit a typical primary headache presentation, they are more susceptible than younger children to stress and environmental influences. Consequently, the clinical characteristics of headaches in pediatric patients can vary with age.
Headaches can be classified as primary or secondary, depending on the underlying etiology. Although life-threatening secondary headaches are rare, some urgent cases require rapid diagnosis and treatment. Therefore, it is crucial to identify patients who necessitate invasive examinations, such as blood tests, cerebrospinal fluid (CSF) analysis, and neuroimaging, to exclude secondary headache. This is achieved through a detailed history and physical examination of patients presenting with headaches, which can save time, effort, and financial resources [3]. In this context, red flags are clinical indicators that signal the need for neuroimaging to identify secondary causes of headaches [1]. Numerous studies have investigated these red flag signs; however, many patients with primary headaches also exhibit these signs, and in some prior cases, the signs have not corresponded to secondary headaches [4]. Moreover, little research has examined whether the application of red flag signs should vary according to patient age.
This study was conducted to facilitate the identification of distinct characteristics of patients with headaches across age groups while exploring the primary diagnostic methods. Therefore, we can determine which patient-reported information should be prioritized during history-taking. Furthermore, we examined which red flag signs are critical for each age group, in an effort to facilitate a more efficient diagnosis.
Materials and Methods
The study focused on patients who presented at the Department of Pediatrics and the emergency room of Pusan National University Hospital between January 2018 and December 2022. We performed a retrospective medical chart review of patients under 18 years of age who cited headaches as their primary concern. We excluded headaches that were attributable to underlying diseases, such as established intracranial lesions or postictal states following seizure.
The data collected included sex, age, patient history, and family history of headaches. We investigated headache characteristics such as the period of symptom onset—defined as the time from the first appearance of symptoms until the patient’s hospital visit (<1 month, 1–6 months, 6 months–1 year, 1–3 years, or >3 years)—as well as the frequency of headaches (less than once a month, 1 to 3 times a month, 1 to 2 times a week, 3 or more times a week, or daily), duration of pain (<1 minute, 1–30 minutes, 30 minutes–1 hour, 1–2 hours, 2 hours–3 days, or >3 days), location (frontal, temporal, parietal, occipital, or not localized), and associated symptoms (anorexia, nausea, vomiting, photophobia, or phonophobia). We also investigated stress factors and findings from neurological examinations. Short stature was defined as a height below the third percentile for the patient’s age and sex, while overweight/obesity was defined as a body mass index at or above the 85th percentile, similarly considering age and sex. Patients reported their headache characteristics using a questionnaire on which they checked each applicable item, and pain intensity was measured with a visual analog scale. Laboratory evaluations included complete blood count, C-reactive protein level, erythrocyte sedimentation rate, thyroid function tests (TFTs), and CSF analysis. TFTs and CSF studies were the most frequently conducted examinations in the patient data set. Results from electroencephalography (EEG) and neuroimaging, which included computed tomography (CT), magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), and magnetic resonance venography (MRV), were also analyzed. EEGs were interpreted by pediatric neurologists, while all neuroimaging studies were interpreted by neuroradiologists.
Age was divided into three groups: group A, pre-school age (<6 years); group B, school-age (6–12 years); and group C, adolescence (>12 years). Additionally, 17 categories were evaluated to determine the presence of red flags: (1) systemic symptoms such as fever; (2) history of neoplasm; (3) sudden headache onset (<1 month); (4) change in headache pattern; (5) positional headache; (6) progressive headache; (7) eye pain with autonomic symptoms; (8) post-traumatic headache onset; (9) vomiting; (10) being awakened from sleep by pain; (11) precipitation of headache by coughing, exercise, or the Valsalva maneuver; (12) headache upon or soon after waking in the morning; (13) lack of response to medical therapy; (14) abnormal neurological signs and symptoms; (15) papilledema; (16) occipital headache; and (17) absences from school or leaving early. Headaches were classified according to the International Classification of Headache Disorders, Third Edition, as proposed by the Committee of the International Headache Society [5]. These were further grouped into primary or secondary headaches. If a headache did not fit a clearly defined type, it was deemed an unclassified headache, which was part of the primary group.
Statistical analyses were conducted using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Differences between age groups regarding clinical symptoms were assessed using the chi-square test, the Fisher exact test, and one-way analysis of variance. A P value of less than 0.05 was considered to indicate statistical significance. For comparisons among the three independent groups, a post hoc analysis using the Bonferroni correction was performed, with a P value of less than 0.0167 denoting statistical significance. The study received approval from the Institutional Review Board of Pusan National University Hospital for research involving human participants and experimental animals (PNUH IRB 2310-013-132). Informed consent was waived by the board.
Results
The study included a total of 687 patients. Table 1 presents the demographic and clinical characteristics of the three age groups. Group A comprised 102 patients, group B included 314, and group C contained 271. Regarding sex, group A included 52 male participants (51%), group B had 161 (51.3%), and group C had 125 (46.1%). No statistically significant differences were observed among the three age groups in terms of sex, past medical history, family history of headache, physical examination findings, TFTs, and results from EEG, brain CT, brain MRI, MRA, or MRV assessments. However, significant differences were noted across the groups in overweight/obesity, the period of symptom onset, headache frequency, pain duration, headache localization, associated symptoms, academic stress, headache type, and CSF examination results. The Bonferroni test was used to compare each pair of groups independently (Table 2). Overweight/obesity was found in two patients (2.0%) in group A, 38 (12.1%) in group B, and 65 (24.0%) in group C. The prevalence of overweight/obesity increased with age, with the highest frequency in adolescence. The period from symptom onset to presentation and the duration of pain were significantly shorter in group A compared to the other groups. Relative to group A, patients in group C were more likely to experience headaches more than three times a week. However, daily headaches were more frequently reported in group A than in the other groups. The rates of nausea, photophobia, and phonophobia were significantly higher in groups B and C compared to group A. In contrast, vomiting was significantly more commonly reported in group A than in the other groups. Academic stress was more prevalent among older patients compared to those younger than 6 years. Secondary headaches were more commonly diagnosed in group A, while primary headaches were more frequent in groups B and C. Among primary headaches, unclassified headache was the most common in all age groups, followed by tension-type headache and migraine without aura. Even excluding unclassified headaches, the proportion of primary headaches was higher in groups B and C, with respective rates of 28.3% and 26.2% compared to 9.8% in group A. Infection-related headache was the predominant type of secondary headache in all groups. In group B, brain lesions were the second most common type, affecting three patients (1.0%); in group C, intracranial hypertension was identified in four patients (1.5%), while thyroid-associated headache, brain lesions, and somatic symptoms and related disorders were each confirmed in three patients (1.1%). The CSF analysis results were also comparable across groups. Pleocytosis was the most frequently observed abnormal CSF test result in all three age groups. Idiopathic intracranial hypertension was identified in 1.0%, 0.3%, and 1.5% of patients in groups A, B, and C, respectively.

Clinical, laboratory, and imaging characteristics of patients categorized by age group
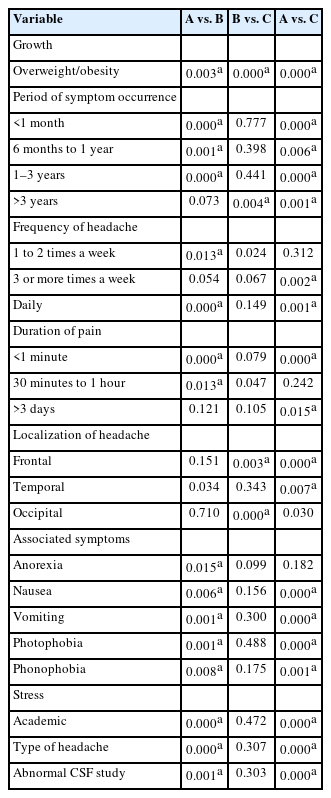
Results of the Bonferroni test among the three age groups
Table 3 illustrates the importance of various red flags in differentiating secondary headaches across age groups. In all age categories, the presence of fever, sudden headache onset, poor response to medication, or accompanying abnormal neurological signs and symptoms tended to indicate secondary headache. In groups A and B, secondary headache was associated with vomiting (P<0.001 for both). However, other factors, such as waking up with a headache (P=0.008); experiencing pain immediately upon waking (P=0.001); precipitation by coughing, exercise, or the Valsalva maneuver (P=0.001); and leaving school early or being absent (P=0.000) more commonly coincided with primary headaches in group B. In group C, primary headaches were more likely to be triggered by coughing, exercise, or the Valsalva maneuver (P=0.001); to involve pain upon waking (P=0.002), and to be associated with school absences or early departures (P=0.000) compared to secondary headaches. The findings suggest that in patients under the age of 12 years, vomiting should raise a strong suspicion of secondary headache, warranting further evaluation with blood tests, imaging, and CSF examination. In contrast, for patients over 6 years old, if the headache worsens with coughing, exercise, or the Valsalva maneuver; occurs after waking; or is associated with school absences or early departures, primary headache is more likely. In such cases, additional testing may not be necessary and should be considered based on individual patient characteristics.
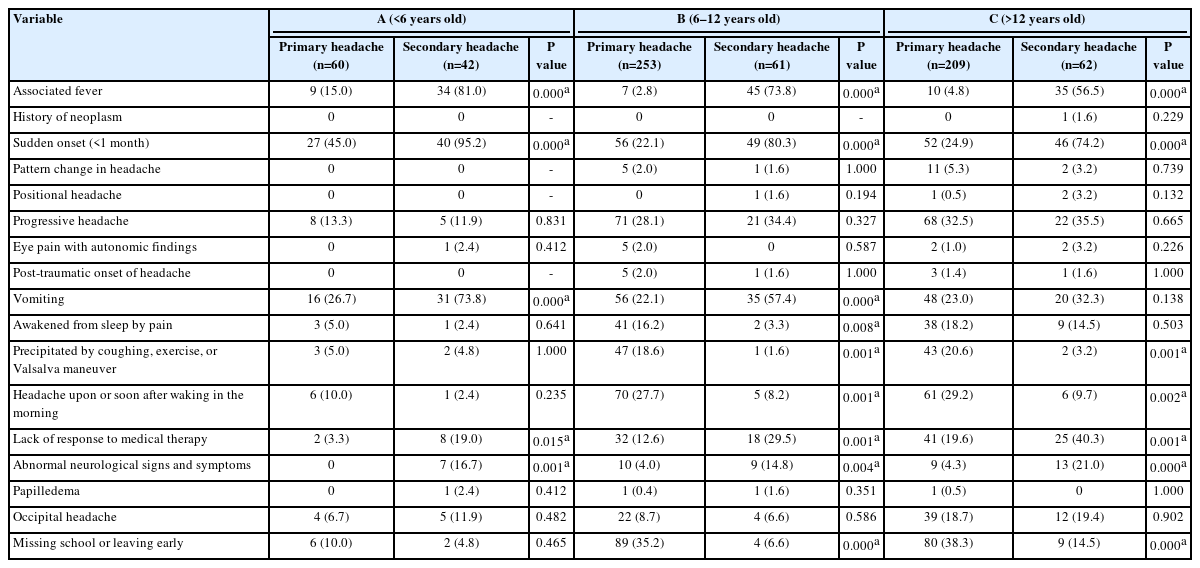
Comparison of red flag signs in primary versus secondary headache by age group
Discussion
In this study, overweight/obesity—a condition known to influence headaches—was confirmed to occur at a higher rate with increasing age, with significant differences observed across age groups. The reported relationship between obesity and headaches has varied among previous studies. While some research has found no correlation between the two [6-8], Ravid et al. [9] reported that migraine was associated with being overweight, with a more pronounced association in female than in male participants. Furthermore, the frequency of headaches has been found to be greater in children with obesity compared to their normal-weight counterparts [9,10]. As individuals age, the prevalence of obesity tends to rise due to various social and environmental factors. This may lead to an increased frequency of both primary and secondary headaches, including those caused by intracranial hypertension related to obesity [11].
In our study, participants were categorized into three age groups: pre-school age, school-age, and adolescence. However, to compare various clinical characteristics, we alternatively categorized the patients into two groups based on the age of headache onset: early-onset, which included children under 6 years of age, and late-onset, which comprised children over 6 years old. This division was useful in revealing more pronounced results. Among the early-onset participants, symptom onset was typically brief, lasting less than 1 month. Conversely, in the late-onset group, symptom onset often extended beyond 6 months. Additionally, a higher number of patients in the early-onset group reported experiencing pain that lasted for less than 1 minute. This finding aligns with previous research indicating that attack duration tends to be shorter with early-onset headaches [2]. However, our study diverged from prior findings in that a greater proportion of patients in the early-onset group reported daily headaches relative to the late-onset group. Patients under 6 years old face challenges in accurately verbalizing their symptoms, and their daily reports of headaches may include behaviors such as facial grimacing and fussing; they may also describe general physical discomfort as a headache [2]. In the late-onset group, we observed high frequencies of nausea, photophobia, and phonophobia. As patients age, they are better able to understand and articulate their symptoms, and they more frequently develop typical primary headaches. Separately, academic stress was markedly higher in the late-onset group. Given that adolescence in Korea is heavily focused on academic achievement, the associated stress likely contributes to headaches. This aligns with findings from a previous Italian study, which identified school as the most influential trigger of headaches in adolescents, corroborating our results [12]. In our data, the early-onset group exhibited a higher frequency of secondary headaches, while the late-onset group had a higher frequency of primary headaches. Childhood headaches were often classified as secondary in nature, with a substantial number related to infection, echoing previous findings [13].
Red flag signs serve as guidelines and recommendations for neuroimaging, yet no clear consensus has been reached regarding which findings should guide decision-making [14]. We evaluated our results in relation to several previous studies that evaluated the diagnostic value of red flag signs for headaches. Table 3 summarizes 17 red flag signs, with headache onset at <6 years of age also considered a red flag. Relative to prior research, our study indicated that headaches beginning before the age of 6 years, abnormal neurological signs or symptoms, systemic symptoms such as fever, and sudden onset were more indicative of secondary headache [1,3,15,16]. However, vomiting was a significant red flag only in patients under 12 years old in our study, while headaches triggered by coughing, exercise, and the Valsalva maneuver were significantly more common among patients over 6 years of age with primary headaches. This result contradicts those of previous studies [1,15]. Moreover, a high frequency of headache upon awakening was reported among patients over 6 years old with primary headaches, contradicting the findings of Yayici Koken et al. [3], who reported that this feature (headache consistenly worse in the morning) was more common with secondary headaches. As headache duration increases, more patients are likely to report experiencing a headache immediately upon awakening. This may also reflect the stress of waking up early for school. Some studies have reported that waking from sleep due to a headache is associated with secondary headache; however, we found no significant relationship [3,15,17]. The onset of headaches before 6 years of age is an important red flag sign. However, we observed no statistical difference in the rate of neuroimaging abnormalities across age groups. Furthermore, in accordance with other studies, our data are compatible with the concept that early-onset headaches are generally benign, and their clinical course or impact generally does not differ from that of headaches beginning during adolescence [2]. The necessity of routine neuroimaging for younger children with headaches has often been discussed. While some previous studies have identified serious neurological disorders, including tumors, in young children with chronic headaches and normal neurological examination findings [18], others have reported that routine neuroimaging in patients with recurrent headaches and normal neurological examinations did not yield significant results [19]. Therefore, young children presenting with headaches should be carefully evaluated for neurological abnormalities and other red flag signs, necessitating a tailored approach for each patient.
In this study, we also considered the detrimental impact of headaches on academic life, which is not commonly evaluated as a red flag sign but represents an important psychosocial factor for children and adolescents. Consistent with the high level of academic stress among patients over 6 years old, we noted a high frequency of departing school early or being absent. Furthermore, the frequency was significantly higher in patients diagnosed with primary headache compared to those with secondary headache. Consequently, lifestyle modifications or psychological support may be necessary to alleviate patient concerns and assist them in maintaining their academic life.
This study had several limitations. First, due to its retrospective design, not all data were available, and missing data may have been underreported during the chart review. Second, as the study was conducted at a tertiary hospital, it likely involved a select group of patients with severe headaches. Consequently, the clinical symptoms of children presenting with headaches would be more thoroughly assessed through larger prospective studies or collaborative trials.
In conclusion, this study compared the clinical characteristics of pediatric patients with headaches across different age groups. While red flags serve as valuable tools for patient evaluation, they do not invariably represent valid warnings. Clinicians should exercise judgment, considering the patient’s age and unique characteristics, to conduct appropriate examinations and determine the necessity for urgent treatment.
Notes
Sang Ook Nam is an editorial board member of the journal, but he was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Author contribution
Conceptualization: YHJ, YJL, DS, and YMK. Data curation: YHJ, YJL, DS, SYL, JK, YJL, SON, and YMK. Formal analysis: YHJ, YJL, DS, SYL, JK, YJL, SON, and YMK. Methodology: YHJ, YJL, DS, and YMK. Project administration: YHJ, YJL, DS, SYL, JK, YJL, SON, and YMK. Visualization: YHJ, YJL, DS, and YMK. Writing - original draft: YHJ. Writing - review & editing: YHJ and YMK.