Assessment of Knowledge, Attitudes, and Practices of Parents/Caregivers towards Migraine in Children: A Cross-Sectional Observational Study
Article information

Abstract
Purpose
This study aimed to evaluate the knowledge, attitudes, and practices (KAP) of parents or caregivers of children suffering from migraines at a tertiary care center in North India.
Methods
We conducted a cross-sectional study involving 100 parents or caregivers, using convenience sampling. A 20-item questionnaire was administered in English and also translated into the local language (Hindi). The study included children with migraines who visited the pediatric outpatient department within a 6-month period (December 2022 to May 2023).
Results
Over 60% of caregivers were aware of the chronic nature of the illness, its triggering factors, the role of family history, and the importance of lifestyle modifications. However, only 46% understood the pathophysiology of the illness, and 53% were aware of the medication used for childhood migraines. More than 85% of caregivers believed that recurrent headaches necessitate a doctor's consultation, may require regular visits for optimal treatment, and were willing to alter their child's lifestyle to prevent headaches. However, a significant percentage of caregivers (47%) practised self-medication for their children's headaches. Most caregivers believed that lifestyle modifications and avoiding triggers were the best treatments for migraines. There were significant associations (P<0.05) between the level of education and responses to questions related to migraine definition, prophylaxis, treatment, investigations, lifestyle modifications, and screen time.
Conclusion
Most participants were well-educated on migraine, and their KAP regarding migraine prevention and treatment were generally adequate. However, the practice of self-medication without professional guidance is a significant concern.
Introduction
Recurrent headaches are not uncommon in children [1]. The most frequently occurring and debilitating primary headache among this group is the migraine, which can significantly impair a child's life and family dynamics. It can also negatively impact their quality of life. Migraines in children exhibit different clinical characteristics compared to those in adults [2]. Unlike in adults, migraines in children typically last longer and are often bifrontal or bitemporal in location. They are less common before the age of three. Before puberty, boys are more frequently affected, but after puberty, the condition primarily affects girls. The pain can range from moderate to severe. There are several potential triggers, and a significant family history is present in the majority of cases [3].
The Paediatric Migraine Disability Assessment Tool (PedMIDAS), a modified version of the Migraine Disability Assessment Test (MIDAS) for adults, can be used to evaluate disability in children and adolescents [4]. The diagnosis of a migraine is typically clinical, but additional testing should be conducted to rule out serious secondary causes. Both pharmacological and non-pharmacological approaches are used for management. The cornerstone of management is parental education and lifestyle modifications. Acute treatment consists of acetaminophen, non-steroidal anti-inflammatory drugs, and triptans [5,6].
The goal of preventive therapy is to reduce the frequency and intensity of headaches. Other effective medications for the pediatric age group include flunarizine, propranolol, amitriptyline, levetiracetam, valproate, and topiramate. A pediatrician should examine the child to rule out secondary causes of headaches when necessary [7].
To improve the quality of life and academic performance of a child suffering from migraines, caregivers must be well-informed about this chronic neurological disorder. However, there is a lack of literature regarding the knowledge, attitudes, and practices (KAP) of parents/caregivers concerning childhood migraines, especially in developing countries like India. Therefore, there is a need to study these factors, as they can significantly impact the management and treatment compliance for migraines in children. The objective of this study was to assess the KAP of caregivers of children with migraine.
Materials and Methods
1. Study design
A descriptive cross-sectional questionnaire-based study was conducted at a tertiary care hospital in northern India from December 2022 to May 2023. Ethical approval for the study was obtained from the Command Hospital, Chandimandir ethical committee (letter number 22/11/CHWC/2022). The written informed consents were taken by all the parents/caregivers.
2. Case selection
The study encompassed children aged between 5 and 18 years who suffered from migraines and were accompanied by parents or caregivers to the pediatric outpatient department (OPD) from December 2022 to May 2023. We screened a total of 120 children with a clinical diagnosis of migraine (as per International Classification of Headache Disorders [ICHD]-3) who visited the OPD. However, 20 were excluded for various reasons, leaving 100 parents or caregivers who completed the questionnaire for the final analysis. The majority of the children had been experiencing symptoms for more than 12 months. We developed a questionnaire by utilising various databases, including Science Direct, Scopus, and PubMed. This questionnaire was subsequently reviewed and refined by experts in migraine management and the Institute's ethics committee. The questionnaire was divided into four sections, each focusing on the subject's demographics, KAP related to migraines (Appendix 1). The inclusion criteria were parents or caregivers who could speak and read English or the local language (Hindi). Those who were unwilling to participate, unable to read and write, or not willing to provide informed consent were excluded. The number of respondents to the English and Hindi questionnaires was 40 and 60, respectively.
3. Statistical analysis
The collected data were recorded in a Microsoft Excel spreadsheet (Redmond, WA, USA). The statistical analysis was performed using SPSS version 20 (IBM Corp., Armonk, NY, USA). Categorical variables were presented as number and percentage, while continuous variables were presented as mean±standard deviation. The chi-square test was used to assess the associations of categorical variables with caregivers’ level of education. A P value <0.05 was considered statistically significant.
Results
During the study period, we screened a total of 120 children with migraines who were accompanied by their parents or caregivers at the pediatric neurology OPD and clinic. Of these, 20 were excluded for various reasons. The final analysis included 100 parents or caregivers who responded to the questionnaire (Fig. 1).
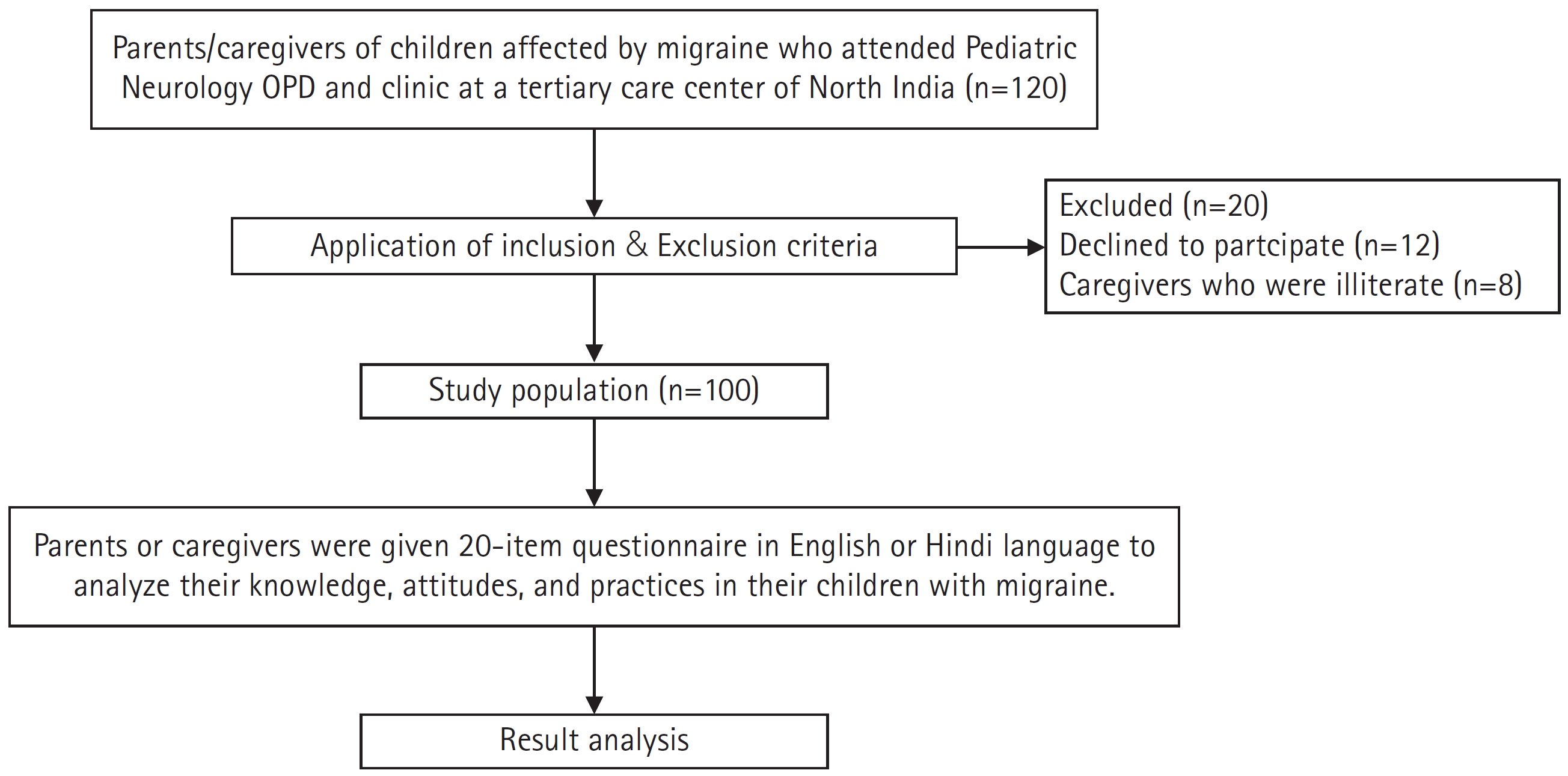
Flow of study. OPD, outpatient department.
The ages of the children with migraine in the study ranged from 5 to 18 years, with an average age of 10.41±2.54. The boys constituted 53%(n=100) and girls 47% respectively. Most of the caregivers had a good level of education, with approximately 83% being graduates or postgraduates (Table 1).
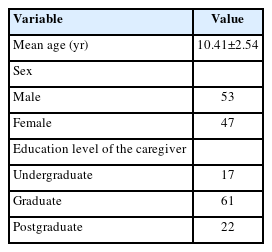
Demographic profile of study participants
1. Evaluation of knowledge about migraine among caregivers
The survey questions related to knowledge about migraines revealed that over 60% of caregivers understood the chronic nature of the illness, its precipitating factors (such as skipping meals, exposure to bright light, stressors, specific food items, and lack of sleep), and the influence of family history and lifestyle modifications. Approximately 57% were aware that the severity of a migraine can dictate the need for migraine prophylaxis, but the majority of caregivers were unfamiliar with the duration of such prophylaxis. Over 60% of caregivers believed that neuroimaging is always necessary for children with migraines. However, around 90% of caregivers were not familiar with the HTP (House, Tree, and Person) psychological test used in relation to migraines (Table 2).
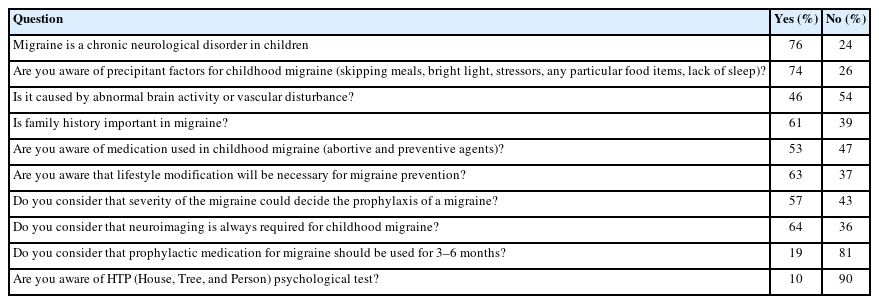
Evaluation of knowledge among caregivers
2. Evaluation of attitudes toward migraine among caregivers
A large majority of caregivers (85%) held the belief that migraines necessitate a consultation with a doctor, and potentially, regular visits for optimal treatment. A substantial proportion of caregivers were willing to modify their child's lifestyle to enhance prevention. However, it is noteworthy that approximately 47% of caregivers engaged in self-medication for their children's headaches (Table 3).

Evaluation of attitudes among caregivers
3. Evaluation of standard practices among caregivers
The majority of caregivers believed that lifestyle modification and avoidance of triggering factors constitute the most effective treatment for migraines. They were also open to undergoing tests for migraines as recommended by their physicians. Furthermore, they were knowledgeable about the latest treatment modalities for migraines, which include newer drugs, cognitive behavioral therapy, yoga, and neuromodulation (Table 4).
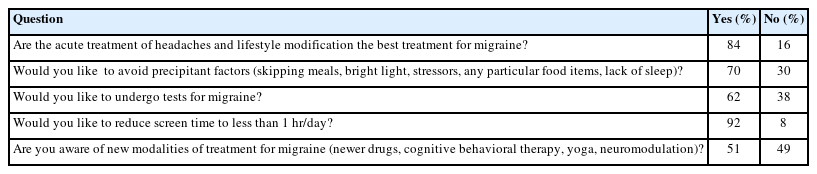
Evaluation of standard practice in study participants
Significant associations (P<0.05) were found between the level of education and questions pertaining to the definition of migraine, prophylaxis, treatment, investigations, lifestyle modifications, and screen time, as compared to other questions related to the KAP of caregivers towards migraine (Table 5).

Association between knowledge, attitudes, and practices of parents/caregiver with level of education
Discussion
Migraines significantly impact a child's intellectual performance, memory, personality, and daily activities. There is a dearth of literature on the prevalence of pediatric headaches and the factors contributing to the recurrence of primary headaches. While questionnaire-based studies offer more reliable information and are feasible, clinical interviews remain the gold standard for such research. Increased awareness of the disease has positively impacted healthcare, leading to a decrease in morbidity and mortality. Previous studies have confirmed that patients' knowledge and awareness dramatically influence medication adherence behavior [8].
Upon reviewing the existing literature, we concluded that our study is the first of its kind to assess the KAP among caregivers of children with migraines. Most of the studies mentioned in the literature focus on adult patients or physicians' knowledge of this chronic neurological disorder. In our study, over 60% of caregivers were aware of the chronic nature of the illness, its precipitating factors (such as skipping meals, bright light, stressors, specific food items, lack of sleep), and the role of family history and lifestyle modifications. This awareness level appears to be much higher compared to other studies, primarily those involving adults [9]. However, only 46% of caregivers understood the pathophysiology of the illness, and 53% were familiar with the medication used for childhood migraines, both abortive and preventive. Our study also revealed that more than 85% of caregivers believed that migraines require a consultation with a doctor, may necessitate periodic visits for better treatment, and were ready to change their children’s lifestyles to prevent headache. This understanding will further assist clinicians in ruling out more serious causes of headaches that require urgent treatment. Our study also found that the majority of caregivers believed that lifestyle modification and avoiding precipitating factors are the best treatments for migraines. This belief was much more prevalent than in other adult studies mentioned in the literature [10-12]. Caregivers also expressed willingness to undergo tests for migraines as per physician advice and were aware of new treatment modalities for migraines. However, a significant percentage of caregivers (47%) practised self-medication for their children's headaches without consulting a doctor, a trend comparable to adult studies mentioned in the literature [13]. This incorrect practice may be due to the availability of over-the-counter drugs and information through social media, which regulatory agencies should address and attempt to curb.
Significant associations (P<0.05) were found between the level of education and questions pertaining to the definition, prophylaxis, treatment, investigations, lifestyle modifications, and screen time related to migraine. This finding underscores the importance of educational level and knowledge about this chronic condition for improving the understanding and treatment of migraines in children.
In conclusion, most of the included participants had a strong educational background, and KAP regarding migraine prevention and treatment were adequate. However, the prevalent issue of self-medication without expert consultation was a significant concern. Health authorities should consider implementing educational programs that provide accurate information, foster positive attitudes, and enhance practical skills related to migraine. This could lead to an improved quality of life for children affected by migraine.
Notes
No potential conflict of interest relevant to this article was reported.
Author contribution
Conceptualization: RS, AKM, and SS. Data curation: RS and AU. Formal analysis: AKM, MU, and AU. Visualization: MU and SS. Writing-original draft: RS, AKM, and MU. Writing-review & editing: RS, AKM, and SS.
Acknowledgements
The authors acknowledge the contribution of all the staff of Pediatric Neurology Division.