Introduction
The estimated lifetime risk of a seizure of any kind is about 8%, and the lifetime risk of epilepsy is approximately 1%; epilepsy is the fourth most common neurological disorder, affecting approximately 50 million people worldwide [1-4]. In children, the prevalence of epilepsy is about 0.3% to 0.5%, and the cumulative incidence of epilepsy is approximately 0.66% at 10 years of age in developed countries [3,5]. Both the prevalence and incidence of epilepsy in children are higher in developing countries [3]. Among seizure types, several population-based studies have consistently reported a slight predominance of focal seizures compared with generalized seizures, making focal seizures the most common seizure type in childhood epilepsy [6-10].
After careful history-taking, electroencephalography (EEG) is the most important investigation for evaluating unprovoked seizures and diagnosing epilepsy. The main purpose of performing EEG in patients with epilepsy is to confirm the presence of interictal epileptiform discharges. A polyspike complex is a sequence of two or more spikes that may or may not be an interictal epileptiform discharge [11]. The association between polyspike complexes and generalized epilepsy has been widely studied, but little is known about the significance of focal (regional) polyspike complexes in patients with focal epilepsy [12,13].
In the current study, therefore, we aimed to investigate the significance of focal polyspikes as interictal epileptiform discharges in patients with focal epilepsy.
Materials and Methods
1. Patients
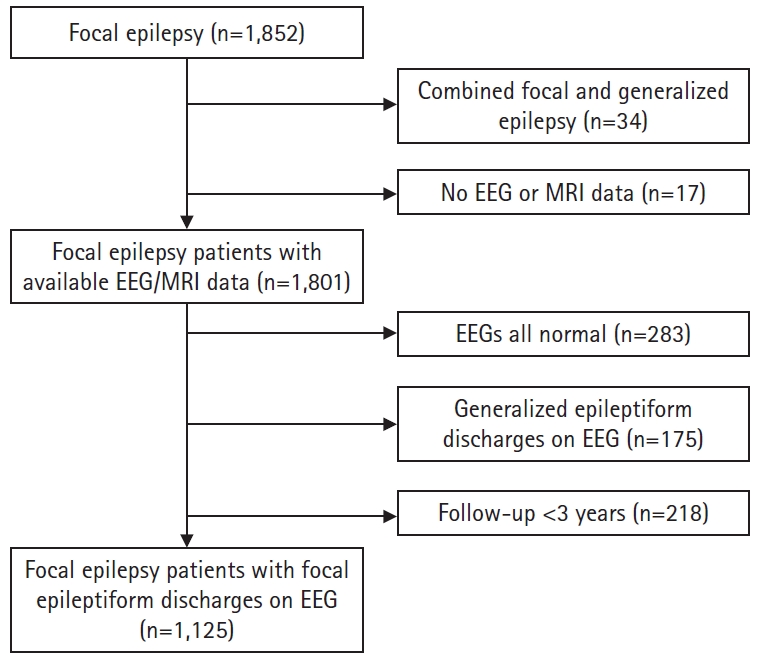
Patients who were diagnosed with focal epilepsy at Pusan National University Children’s Hospital between 2009 and 2016 were retrospectively extracted from the patient database. The inclusion criteria were as follows: (1) patients who were diagnosed with focal epilepsy and received anti-seizure medications (ASMs) at Pusan National University Children’s Hospital between 2009 and 2016; (2) patients <18 years of age at the time of diagnosis; (3) patients whose EEG and brain magnetic resonance imaging (MRI) data were available; and (4) patients with a follow-up period of >3 years since the initiation of ASMs. Patients without EEG or brain MRI data were excluded. Patients with only normal EEGs (i.e., no epileptiform discharges on any EEGs in patients with repetitive EEG examinations; non-epileptiform abnormalities were neglected for the purposes of this study, and patients with only non-epileptiform abnormalities on all EEGs were considered as having normal EEGs) were also excluded. Then, patients who showed generalized epileptiform discharges at least once on their EEGs were excluded. Therefore, focal epilepsy patients with identified focal epileptiform discharges on their EEGs and available MRI data were finally included in this study (Fig. 1).
Clinical variables such as sex, age at diagnosis, age at seizure onset, the presence of a comorbid intellectual disability, and brain MRI findings were collected. Seizure frequencies at the time of diagnosis, and at 1, 2, and 3 years after the diagnosis were also collected, which reflected the average of seizure frequencies during the immediate previous 1-year period. The number of ASMs prescribed at 1, 2, and 3 years after the diagnosis was also obtained.
Patients were defined as having a structural etiology if their brain MRI examinations were interpreted as abnormal by pediatric radiologists and these abnormal findings were considered as the epileptogenic foci by the treating pediatric neurologists. The abnormal brain MRI findings that were considered irrelevant by the treating pediatric neurologists were again reviewed for confirmation. Patients with brain MRI abnormalities that were irrelevant to epilepsy were considered as having negative MRI results.
Patients were defined as having drug-resistant epilepsy if they failed to achieve seizure freedom for more than 1 year after trials of two adequate ASMs of more than 2 years. We also recorded whether patients received treatment modalities other than ASMs, such as a ketogenic diet or epilepsy surgery, and the presence of an intellectual disability as a comorbidity.
This study was approved by the Institutional Review Board of Pusan National University Yangsan Hospital (IRB No. 2021-0159). The requirement to obtain informed consent from the patients or caregivers was waived due to the retrospective nature of this study.
2. EEGs
The patients’ EEGs were examined using an EEG monitoring system with electrodes placed according to the international 10 to 20 system with a duration of at least 30 minutes. Existing interpretations of EEGs by one of the two pediatric neurologists (YJL and SON) were compared with interpretations performed by a third pediatric neurologist (AK), who was unaware of the clinical information of the patients. In case of disagreement (three patients), a fourth pediatric neurologist (JK), who was also unaware of the clinical information of the patients, interpreted the EEGs. All pediatric neurologists who participated in EEG interpretations were certified by the Korean Board of EEG and Clinical Neurophysiology. Interpretations were selected if two neurologists gave concordant findings.
Patients without any interictal epileptiform discharges were excluded, as described above. Epileptiform discharges were defined as waveforms fulfilling at least four of the following six criteria, following the guideline proposed by the International Federation of Clinical Neurophysiology (IFCN): (1) di- or tri-phasic waves with a sharp morphology; (2) different wave duration than the ongoing background activity; (3) asymmetry of the waveform (a sharply rising ascending phase and a more slowly decaying descending phase, or vice versa); (4) transient followed by an associated slow after-wave; (5) disrupted background activity surrounding epileptiform discharges; and (6) distribution of the negative and positive potentials on the scalp suggesting a source of the signal in the brain [11]. Patients who showed such epileptiform discharges at least once on their serial EEGs were included in this study.
3. Polyspikes and patient grouping
In order to differentiate polyspikes from paroxysmal fast activities, which last longer than polyspikes, with a duration of >0.25 to 0.5 seconds, polyspikes were defined as sequences of two or more epileptiform discharges (sharp waves or spikes) lasting 0.5 seconds or less [14,15]. Patients who only showed paroxysmal fast activities on their EEGs without polyspikes were not considered as patients with polyspikes. Polyspikes appearing during the ictal phase were also excluded.
Patients were divided according to the presence of polyspikes on their EEGs. Patients who showed one or more polyspikes on any of their past EEGs were classified as the polyspike-positive group. Patients who never showed polyspikes on their EEGs were classified as the polyspike-negative group.
Patients with both a structural etiology on brain MRI and polyspikes on EEG were further divided into the localized polyspike spike and the multifocal polyspike group. The localized polyspike group was defined as patients whose polyspikes on EEGs were only present within the locations of epileptogenic structural lesions on their brain MRI examinations. The term “multifocal” was used differently from its typical meaning in this study. The multifocal polyspike group was defined as patients whose polyspikes on EEGs were distinctively present in locations other than the structural lesions shown on their brain MRI examinations.
4. Statistical analyses
Data are presented as number (percent, %) or median (interquartile range [IQR]). The clinical characteristics of the polyspike positive and polyspike negative groups were compared using univariate binary logistic regression. Multivariate logistic regression was then used for parameters with P values <0.05 in univariate logistic regression. Subgroup analyses among patients with brain MRI abnormalities were done using the chi-square test or the Fisher exact test. A P<0.05 was considered to indicate statistical significance. SPSS version 23.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses.
Results
1. Demographics and comparison of patients with and without polyspikes: univariate analysis
In total, 1,801 patients <18 years of age were diagnosed with focal epilepsy, evaluated with EEG and brain MRI, and received ASMs at Pusan National Children’s Hospital between 2009 and 2016. Among them, 283 patients were excluded because they never showed any interictal epileptiform discharges on their EEGs (median number of EEGs, 7; IQR, 4 to 11). Furthermore, 175 patients were excluded because they showed generalized interictal epileptiform discharges on their EEGs at least once, and 218 patients were further excluded as they had follow-up periods of less than 3 years. Finally, the remaining 1,125 patients were included in the analysis (Fig. 1).
Among the 1,125 focal epilepsy patients included in the analyses, 468 (41.6%) patients showed focal polyspikes on their EEGs at least once during a follow-up period of more than 3 years (Fig. 2). These 468 patients were classified as the polyspike-positive group, and the remaining 657 (58.4%) patients comprised the polyspike-negative group. All patients in the polyspike-positive group also showed other epileptiform discharges such as spikes or sharp waves on their EEGs.
In the univariate analysis, there was a significant difference in sex (P=0.046) between the polyspike-positive and polyspike-negative groups (Table 1). The patients in the polyspike-positive group were significantly younger at seizure onset (P=0.008) and diagnosis (P=0.008). The polyspike-positive group also contained a significantly larger proportion of patients who had a structural etiology (P<0.001) and a comorbid intellectual disability (P<0.001). Baseline seizure frequency (P=0.006), and seizure frequencies at 1 year (P<0.001), 2 years (P<0.001), and 3 years (P<0.001) after the diagnosis were all significantly more frequent in the polyspike-positive group. Similarly, patients in the polyspike-positive group took a significantly greater number of ASMs at 1 year (P<0.001), 2 years (P<0.001), and 3 years (P<0.001) after the diagnosis. Significantly more patients in the polyspike-positive group were diagnosed with drug-resistant epilepsy (P<0.001), and therefore significantly more patients had tried treatment modalities other than ASMs, such as a ketogenic diet or surgery (P=0.001). No significant difference was found between the polyspike-positive and polyspike-negative groups in the number of EEGs taken during the follow-up period.
3. Comparison of patients with and without polyspikes: multivariate analysis
Multivariate logistic regression was then performed for relevant parameters that showed significant differences (P<0.05) between the polyspike-positive and polyspike-negative groups in univariate logistic regression (Table 2). Age at seizure onset, age at diagnosis, presence of brain MRI abnormalities, presence of intellectual disability, baseline seizure frequency, and presence of drug-resistant epilepsy were clinical variables included in the multivariate analysis. In the multivariate analysis, only the presence of a detectable structural etiology on brain MRI was significantly associated with the presence of polyspikes on EEGs, as more patients with polyspikes than patients without polyspikes had a structural etiology (odds ratio, 10.003; 95% confidence interval, 6.109 to 16.379; P<0.001). In other words, patients with polyspikes were approximately 10 times more likely to have a structural etiology than patients without polyspikes.
4. Presence of polyspikes on EEGs according to specific brain MRI abnormalities
Brain abnormalities were found in 408 patients, and the structural abnormalities could be categorized as follows: hypoxic-ischemic encephalopathy (n=157, 38.5%), destructive encephalomalacia (n=122, 29.9%), focal cortical dysplasia (FCD; n=39, 9.6%), malformation of cortical development other than FCD (n=25, 6.1%), previous infarction (n=21, 5.1%), hippocampal sclerosis (n=13, 3.2%), tuberous sclerosis (n=11, 2.7%), brain tumor (n=9, 2.2%), and others (n=11, 2.7%). Among the 324 patients with polyspikes, hypoxic-ischemic encephalopathy (n=127, 39.2%) and encephalomalacia (n=105, 32.4%) were the most frequent etiologies, followed by FCD (n=35, 10.8%).
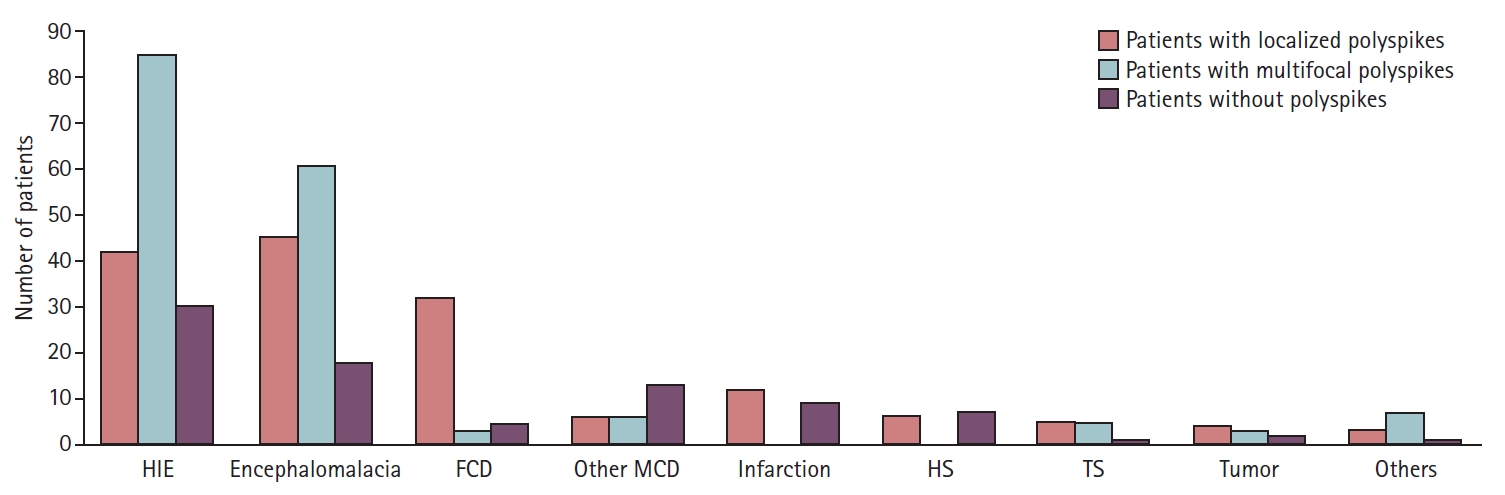
Patients with brain abnormalities were divided into three groups: patients with localized polyspikes (n=155, 38.0%), patients with multifocal polyspikes (n=169, 41.4%), and patients without polyspikes (n=84, 20.6%) according to the criteria described in the Methods section. The types of structural abnormalities significantly differed among the three groups (P<0.001) (Fig. 3).
Among the 408 patients with brain MRI abnormalities, there was a significant difference in types of structural abnormalities between patients with localized polyspikes (n=155) and the other patients (P=0.026); specifically, FCD was more frequent in patients with localized polyspikes (82.1% vs. 17.9%). Among the patients with brain MRI abnormalities, there was also a significant difference in the types of structural abnormalities between patients with multifocal polyspikes (n=169) and the other patients (P=0.010), with multifocal polyspikes most frequently being seen in patients with hypoxic-ischemic encephalopathy and destructive encephalomalacia.
When patients with structural etiologies were compared according to the presence of localized or multifocal polyspikes, a significant difference in the types of structural etiologies was observed (P=0.021). FCD, previous infarction, and hippocampal sclerosis were more frequently seen in patients with localized polyspikes, while hypoxic-ischemic encephalopathy and destructive encephalomalacia were more frequently seen in patients with multifocal polyspikes.
Discussion
In this study, we demonstrated that focal epilepsy patients with interictal polyspikes were significantly more likely to have structural etiology visible on brain MRI. Concordant localized interictal polyspikes with structural lesions showed a significant positive association with FCD, while multifocal interictal polyspikes were significantly associated with hypoxic-ischemic encephalopathy or encephalomalacia.
Although many studies have addressed the significance of polyspikes in generalized epilepsy, there is a paucity of literature on polyspikes in focal epilepsy [12,16]. Noachtar et al. [12] performed a data search for the term “regional polyspikes” in focal epilepsy patients who underwent continuous video-EEG monitoring for 3 to 14 days as a pre-surgical evaluation. Among the 513 patients, 29 showed interictal regional polyspikes, and cortical dysplasia was significantly more frequently identified as the etiology in patients with regional polyspikes [12]. Another study by Noli et al. [16] investigated the EEG features of 31 pediatric patients with FCD type II, and found that nearly half of the patients showed rhythmic spikes and polyspike discharges as interictal abnormalities. Both of these studies concordantly showed that localized (regional) interictal polyspikes could be frequently seen in focal epilepsy patients with FCD as the etiology of epilepsy [12,16]. Those results are in accordance with the findings of the current study, where the interictal polyspikes were significantly more frequently seen in focal epilepsy patients with a structural etiology.
However, unlike previous studies, we investigated both localized (regional) and multifocal polyspikes in focal epilepsy patients, and found that localized interictal polyspikes were more frequently seen in patients with FCD, while multifocal interictal polyspikes were more frequently seen in patients with perinatal insults (hypoxic-ischemic encephalopathy and encephalomalacia). Therefore, the presence of polyspikes on EEGs can serve as a marker of the presence of a structural etiology.
It is known that epilepsy patients with structural, metabolic, or genetic etiologies (previously categorized as symptomatic epilepsy) have poorer prognoses than patients with no identifiable etiology (previously categorized as idiopathic epilepsy) [17]. This may especially be true in children, where many benign focal epilepsy syndromes, such as childhood epilepsy with centrotemporal spikes, Panayiotopoulos syndrome, and Gastaut-type childhood occipital epilepsy, constitute the majority of cases of “idiopathic” focal epilepsy [18]. In this context, based on the findings of the current study, where focal epilepsy patients with interictal polyspikes were significantly more likely to have a structural etiology, it can be concluded that childhood focal epilepsy patients with interictal polyspikes will show poorer prognoses than those without interictal polyspikes. This assumption was supported by the present study findings, insofar as patients with interictal polyspikes had more frequent seizures and took more ASMs than patients without interictal polyspikes during follow-up. However, the multivariate analysis confirmed that these findings were secondary to the presence of a structural etiology.
The significance of spikes, sharp waves, or polyspikes observed on EEG is that they are strongly suggestive of an underlying epileptic disorder. Spikes and sharp waves are thought to have the same physiological significance: they are interictal epileptiform discharges, and therefore used as a marker for epileptogenesis, either focal or generalized, and are suggestive of an underlying tendency toward seizures [19]. The significance of polyspikes has not been clearly delineated. Polyspikes are observed in many generalized seizure disorders, and they may act as ictal discharges in association with clinical myoclonic jerks. As polyspikes in genetic generalized epilepsy are reported to be associated with prolonged seizures or drug-resistant epilepsy, they may represent more active or severe epileptic activity [20,21]. This may explain the observation of the present study that focal polyspikes were associated with structural epilepsy, as structural epilepsy is known to produce more severe, and possibly more frequent seizures, which are harder to control than those in patients with non-structural epilepsy. However, further studies are needed to obtain more robust support for this hypothesis. The cellular mechanisms behind the generation of polyspikes in patients with lesional epilepsy, including FCD, are still unknown but probably multifactorial [22]. Studies have shown that FCD lesions have recurrent excitation and decreased inhibition compared to adjacent non-dysplastic areas, contributing to the generation of prolonged trains of epileptic activity [23,24].
This study demonstrates that focal polyspikes can be used as markers of the possible presence of a structural etiology in routine practice. However, this study also has several limitations. First, polyspikes are sensitive, but not specific, for the above-mentioned etiologies. Furthermore, due to the retrospective nature of this study, the EEG follow-up intervals of the included patients were not uniform. This may have caused bias, as patients with poor seizure control tend to receive more frequent EEG investigations to evaluate their current states. Patients with structural etiologies usually have poor seizure control, leading to more frequent EEG examinations, which in turn may increase the likelihood of polyspike detection. However, there was no significant difference in the number of EEGs taken between patients with and without interictal polyspikes, reducing the likelihood that this concern posed a substantial issue. Moreover, patients were evaluated with short-term EEG recordings with a duration of 30 minutes. Therefore, interictal polyspikes may have been unnoticed in some patients. To overcome these limitations, a prospective study with regular long-term EEG monitoring is necessary.