Characteristics of Meningitis in Febrile Infants Aged ≤90 Days
Article information

Abstract
Purpose
This study evaluated the clinical and laboratory characteristics of infants ≤90 days old with meningitis who presented to the hospital with a fever. We also investigated whether initial C-reactive protein levels and white blood cell counts were reliable predictors of bacterial meningitis.
Methods
The medical records of 1,151 infants aged ≤90 days who visited our hospital with a fever between October 2009 and October 2019 were retrospectively evaluated.
Results
Of the 1,151 patients, 274 (23.8%) had meningitis (bacterial, n=7; viral, n=206; pleocytosis in the cerebrospinal fluid, n=136). Thirty-seven viral meningitis patients (18.0%) had a positive polymerase chain reaction result without pleocytosis in the cerebrospinal fluid. The patients without pleocytosis were significantly younger. Among the patients with only pleocytosis, 46 had a urinary tract infection, 22 had other viral infections, and the etiology was unknown in 68. Among patients with urinary tract infections, infants without pleocytosis were younger than those with pleocytosis. Low white blood cell counts (<5,000/mm3) were more frequently found in bacterial meningitis patients (n=7) than in viral meningitis patients. Furthermore, there were normal C-reactive protein levels (42.9%) and no pleocytosis (20%) in some cases of bacterial meningitis.
Conclusion
Our findings show that meningitis is not uncommon among infants ≤90 days old who were brought to the hospital with complaints of fever. Furthermore, younger patients may not have cerebrospinal fluid pleocytosis, even if they have bacterial meningitis. Therefore, the patient’s condition should be monitored closely and, if necessary, a re-examination should be considered.
Introduction
Fever is the most common symptom indicative of serious infections among young infants, including neonates [1]. Although most febrile young infants have simple viral infections [2], bacterial infections, such as urinary tract infections (UTIs), meningitis, and bacteremia, are not uncommon.
Central nervous system infections, such as bacterial or viral meningitis, frequently occur in young infants due to immature humoral and cellular immunity. Depending on the age at diagnosis, type of identified organism(s), and delay in treatment, central nervous system infections can lead to several acute comorbidities, severe complications, and long-term disabilities, ranging from hearing loss to a permanent motor or cognitive impairment [3]. An early diagnosis of meningitis in younger infants is essential for correct treatment so as to reduce mortality and complications.
Clinical signs and symptoms of central nervous system infections are often nonspecific in young infants. These symptoms include fever, hypothermia, food retention, skin lesions, irritability, or general malaise [4,5]. Therefore, blood and cerebrospinal fluid (CSF) analyses are performed to diagnose or rule out severe central nervous system infections. A lumbar puncture (LP) with an analysis of the CSF profile might help the clinician differentiate between the presence or absence of meningitis and between bacterial or viral meningitis. CSF white blood cell (WBC) counts >1,000 cells/mm3 suggest bacterial meningitis [6]. The presence of CSF pleocytosis is usually diagnosed with meningitis. However, the absence of CSF pleocytosis in younger infants with enteroviral meningitis has been previously reported [7-9].
In addition, serum C-reactive protein (CRP) levels, WBC count, and procalcitonin are commonly used inflammatory biomarkers in the blood. However, there is no consensus regarding their ability to distinguish between bacterial and viral meningitis [10].
In this study, we aimed to describe the biochemical characteristics of CSF, blood, and urine in febrile infants ≤90 days old with meningitis. Furthermore, we compared the characteristics of the laboratory results in patients with meningitis after dividing them into two groups based on the presence or absence of pleocytosis in the CSF.
Materials and Methods
1. Study population
The medical records of 1,172 patients of age less than 90 days who visited Inje University Sanggye Paik Hospital with a complaint of fever between October 2009 and October 2019 were retrospectively evaluated. The study protocol was approved by the Institutional Review Board of Inje University Sanggye Paik Hospital (2020-03-015). The requirement for informed consent was waived due to the retrospective nature of the study.
Patients <35 weeks gestational age (n=7) and those with underlying conditions (n=14), including Cornelia de Lange syndrome (n=1), cerebral infarction (n=2), periventricular leukomalacia (n=1), Prader-Willi syndrome (n=1), congenital cytomegalovirus infection (n=1), and congenital hypothyroidism (n=1), were excluded. Data regarding age, gestational age, sex, clinical characteristics, diagnosis, and all laboratory profiles, including blood, CSF, urine, and sputum were collected from all the patients.
2. Laboratory tests and microbiological tests of CSF, blood, urine, and sputum
For all included patients, all blood laboratory tests including initial WBC and CRP level checks were performed immediately after visiting the hospital. The peak CRP was defined as the highest numerical value by comparing all tests performed during hospitalization, including the initial CRP.
For all the included patients (n=1,151), LP is usually performed after the initial blood test following which the platelet level is confirmed. In our study, LP was performed on 867 patients (74.3%). Of those 867 patients, 281 did not undergo CSF analysis due to traumatic tap or insufficient sample quantity, and one patient had a positive result for virus polymerase chain reaction (PCR) of enterovirus. Patients with traumatic LP were excluded from the CSF analysis. The detailed results are described in Fig. 1.

Flow diagram depicting the selection of the study population.
All patients who received the LP were tested for bacterial culture and underwent real-time multiplex PCR (Seegene Inc., Seoul, Korea) for six types of viruses—cytomegalovirus, human herpesvirus 6, Epstein-Barr virus, herpes simplex viruses 1 and 2, and varicella-zoster virus—or Reverse Transcriptase PCR for enteroviruses (Seegene Inc.).
Bacterial meningitis was defined as bacterial growth in the CSF. Viral meningitis was defined as either a positive PCR result or patients with age-adjusted CSF pleocytosis with a negative CSF culture or PCR results for a virus without UTIs or bacteremia. Coinfections were defined as meningitis accompanied by bacteremia, UTI, or other viral infections.
CSF pleocytosis was defined as a CSF WBC count >22 WBCs/mm3 if the patient was <4 weeks old; >15 WBCs/mm3 if the patient was between 4 and 7 weeks of age; and >5 WBCs/mm3 if the patient was ≥8 weeks old. UTI was diagnosed as a urine culture (collected by urethral catheterization) with more than 100,000 colony-forming units/mL [11]. The growth of bacteria that are not commonly considered as pathogens (Staphylococcus epidermidis or coagulase-negative Staphylococcus) was classified as a priori as contamination [12].
Patients with various types of meningitis were compared and analyzed based on the presence or absence of pleocytosis in the CSF.
3. Statistical analysis
Continuous variables, including age and CRP, are expressed as the mean±standard deviation and were compared using t-tests. Categorical variables, including sex and age group, were compared using a chi-square test or Fisher’s exact test. The comparison between the viral meningitis group and bacterial meningitis was performed a nonparametric test, Mann-Whitney U test. All statistical analyses were performed using IBM SPSS Statistics for Windows version 25.0 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as a P<0.05.
Results
1. Characteristics of all included patients
During the study period, 1,151 infants (630 [54.74%] males and 521 [45.26%] females) were included. The cause of infection was identified in 724 (432 [59.67%] males and 292 [40.33%] females). LP was performed on 867 patients: meningitis (n=274, 23.8%); UTI (n=180); bacteremia (n=24); and other viral infections (n=347). The remaining 503 patients with unexplained fever were suspected of having a viral infection and they recovered without complications (Fig. 2).
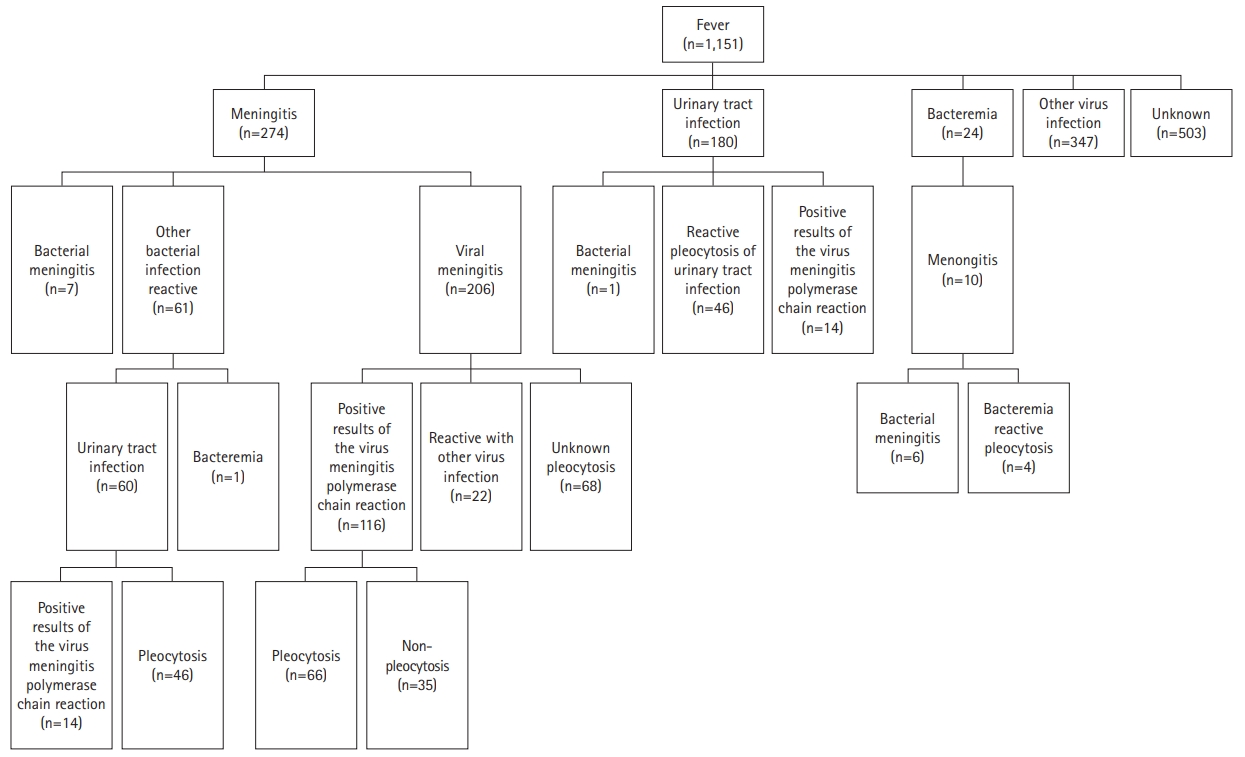
Flow diagram illustrating the strategy to identify the cause of fever.
2. Characteristics of patients with all kinds of meningitis
Of the 274 meningitis patients, 158 (57.7%) were males and 116 (42.3%) were females. The mean age at symptom onset was 52.85±23.42 days (range, 1 to 90). Fifty-nine (21.5%) infants were ≤30 days old, 94 (34.3%) were 31 to 60 days old, and 121 (44.2%) were 61 to 90 days old. Seven patients had bacterial meningitis (Group B Streptococcus [GBS], n=5; Escherichia coli, n=2), 206 had viral meningitis, and 136 had only pleocytosis in the CSF (Table 1). Of the 130 patients with viral meningitis who had a positive viral PCR test, 37 (17.9%) had a positive PCR result without pleocytosis in the CSF. Of the 136 patients with meningitis with only pleocytosis, 46 had a UTI, 22 were reactive in other viral infections, and 68 were of an unknown etiology. The detailed information is described in Fig. 2.
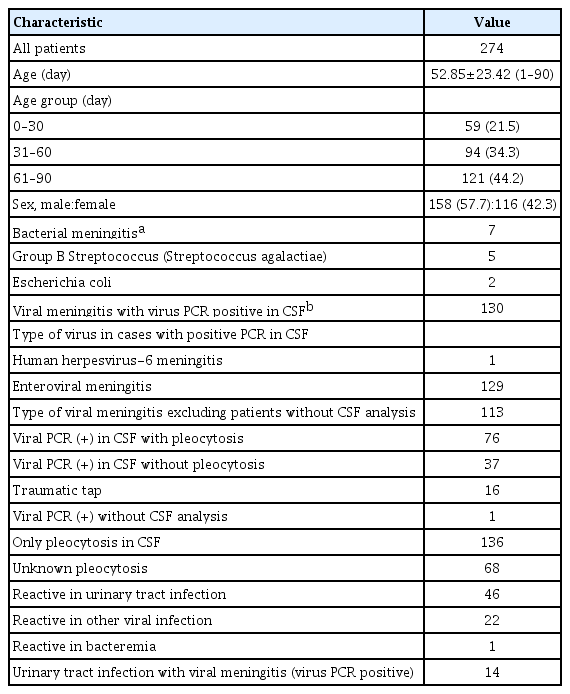
Clinical characteristics of febrile infants with meningitis (n=274)
3. Bacterial infections
Among the patients with bacterial meningitis, except for two patients with traumatic tap who could not be included in the analysis, 80% (4/5) had pleocytosis and 20% (1/5) had non-pleocytosis CSF. One patient who had non-pleocytosis with the initial WBC count and initial CRP in a normal range was later diagnosed with GBS meningitis. In addition, another patient with traumatic tap had CSF non-pleocytosis (CSF red blood cell count, >20,000/mm3; CSF WBC, 3/mm3). Therefore, 28.6% (2/7) of bacterial meningitis patients had non-pleocytosis.
A comparison of the bacteremia patients with and without pleocytosis in the CSF revealed that a significantly large proportion of patients without pleocytosis underwent LP <24 hours after the onset of fever (10/11, 90.9%; chi-square test, P=0.046).
4. Comparison of viral meningitis with and without CSF pleocytosis
Of the 191 children diagnosed with viral meningitis without traumatic tap, 81.7% (156/191) had CSF pleocytosis and 18.3% (35/191) had CSF non‐pleocytosis (Table 2). The comparison of viral meningitis with and without pleocytosis showed no significant difference in CRP (Table 2). However, patients without pleocytosis were significantly younger (39.20±22.64 days vs. 54.19±22.16 days, t-test P<0.05) and had lower WBC counts (12,757±5,358.75/mm3 vs. 9,134±3,507.66/mm3, t-test P<0.05). A greater proportion of patients without pleocytosis underwent LP <24 hours after the onset of fever (chi-square test, P=0.006) than patients with pleocytosis (Table 2). The multivariate logistic regression analysis showed that younger age, shorter interval from fever onset to LP, lower WBC in the peripheral blood, lower CSF protein, and higher CSF glucose were independent predictors of CSF non-pleocytosis in viral meningitis in infants ≤90 days old (Table 2).

Comparison of viral meningitis with and without pleocytosis in cerebrospinal fluid
There were no patients with bad prognosis from viral meningitis. However, one of the patients with bacterial meningitis died and one suffered from subdural empyema, but is developing normally without any sequelae.
5. Characteristics of patients with UTIs
Among the patients with UTIs, 7.8% had coinfection with PCR-positive viral meningitis, 25.6% had reactive pleocytosis in the CSF, and one patient (0.5%) had a co-infection with bacterial meningitis. A comparison of the patients with UTI with and without pleocytosis in the CSF revealed that younger patients had a low rate of pleocytosis occurrence (56.23±20.41 days vs. 67.61±13.59 days, t-test P<0.05). A greater proportion of patients without pleocytosis underwent LP <24 hours after the onset of fever (chi-square test, P=0.001) compared to patients with pleocytosis. This further indicates that younger age and early examination correlate with the absence of pleocytosis.
6. Comparison between bacterial and viral meningitis
When comparing bacterial meningitis with viral meningitis, there were more cases of WBC count <5,000/mm3 in patients with bacterial meningitis (chi-square test, P<0.05) (Table 3). Moreover, the initial CRP levels (0.50 mg/dL [0.3–11.3] vs. 1.00 mg/dL [0.3–13.9], respectively; Mann-Whitney U test, P=0.024) (Table 3) and peak CRP levels (0.60 mg/dL [0.3–14.7] vs. 12.90 mg/dL [6.8–26.7], respectively; Mann-Whitney U test, P=0.000) (Table 3) were significantly different. Initial WBC counts <5,000/mm3 were more frequent in bacterial meningitis cases but CRP levels were significantly different between viral and bacterial meningitis. However, among bacterial meningitis (n=7), three patients (42.9%) had normal CRP level initially.
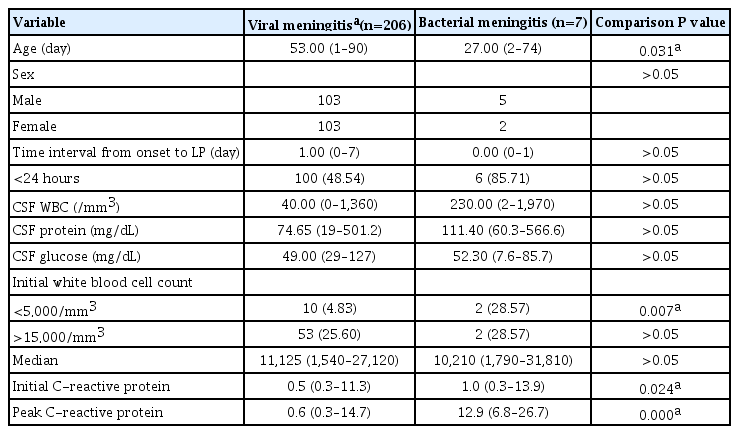
Comparison between viral meningitis and bacterial meningitis patients
Discussion
It is challenging to differentiate between severe infection and benign viral infections among infants aged ≤90 days reporting with a fever. Of the severe infections in young infants, central nervous system infections are the most serious as they may lead to long-term morbidities. However, the most common infection of the central nervous system is aseptic meningitis. In a study of young infants with acute meningitis, almost 80% of infants were found to have aseptic meningitis [3]. In our study, 274 patients (31.6%) were diagnosed with meningitis. Of these, seven had bacterial meningitis, 206 had viral meningitis, and 68 had pleocytosis in the CSF with an unknown cause (Table 1 and Fig. 1).
Of the 191 children diagnosed with viral meningitis without traumatic tap, 18.3% had CSF non‐pleocytosis. In particular, infants with CSF non‐pleocytosis were younger than those with CSF pleocytosis, suggesting a negative correlation with age (Table 2). Univariate analysis showed that a shorter interval from symptom onset to LP, lower CSF glucose, and lower WBC count in the peripheral blood were significantly associated with viral meningitis with CSF non‐pleocytosis (Table 3). In our study, 28.6% of bacterial meningitis patients did not have pleocytosis; however, the number of patients was too small to compare pleocytosis and no pleocytosis. Thus, it might be challenging to differentiate between bacterial and viral meningitis based on initial CSF analysis, as there might be overlaps in the CSF white cell count.
Previous studies also showed some cases of enteroviral meningitis without pleocytosis [7]. The proportion of patients with CSF non‐pleocytosis in the case of enteroviral meningitis was approximately 30% of infants <2 months of age in New Zealand [13] and in Missouri (USA) [14], and 31% in Pennsylvania (USA) [15]. In Korea, approximately 28% of infants <3 months of age [16], 63.3% of neonates, and 38.3% of young infants aged 29 to 56 days [8] had CSF non-pleocytosis in enteroviral meningitis. Mulford et al. [17] reported that 30% of infants <2 months of age with enteroviral meningitis did not have pleocytosis. Although studies published so far have focused upon enteroviral meningitis and CSF pleocytosis, this study shows that various types of meningitis and not only meningitis caused by an enterovirus, may be related to meningitis without CSF pleocytosis in younger patients who were ≤90 days old.
The mechanism of meningitis with non-pleocytosis in infants is still unclear. Seiden et al. [9] reported that CSF non‐pleocytosis is associated with lower peripheral WBC counts and suggested this may result from a lack of sufficient cellular response to infections.
In our study, the mean time interval from onset to LP was significantly shorter in viral meningitis without pleocytosis. These results suggest that sufficient time may be needed for CSF pleocytosis to develop. In other words, in the early stages of central nervous system infections, results may indicate non-pleocytosis if sufficient time has not passed to allow pleocytosis to develop [8,18,19].
Our study showed that 7.8% of UTI patients had coinfection with PCR-positive viral meningitis, 25.6% had reactive pleocytosis in CSF, and one patient (0.5%) had bacterial meningitis (E. coli). Previous studies have shown that sterile CSF pleocytosis is not rare in infants with a UTI undergoing LP (18% to 29% of patients); however, UTIs are rarely associated with bacterial meningitis [20,21]. It is thought that pleocytosis is a type of inflammatory response to UTI and is the result of undetected viral infections [22,23]. In this study, among the patients with UTIs, infants without pleocytosis were younger than those with pleocytosis. It is unknown whether sterile CSF pleocytosis in UTIs is significant and further research on this topic is warranted.
Meningitis may not always be accompanied by pleocytosis. Pleocytosis can be related to age, the interval from symptom onset to LP, and peripheral WBC counts. A comparison between viral meningitis and bacterial meningitis revealed that there were more cases of WBC count <5,000/mm3 in patients with bacterial meningitis (chi-square test, P<0.05) (Table 3). This suggests that bacterial meningitis may present with relatively low WBC counts. Furthermore, CSF non-pleocytosis may also be present. Although the initial CRP levels were significantly different between viral and bacterial meningitis (0.50 mg/dL [0.3–11.3] vs. 1.00 mg/dL [0.3–13.9], respectively; Mann-Whitney U test, P=0.024) (Table 3), initial CRP levels were normal in three cases of seven bacterial meningitis (3/7, 42.9%). Together, these results suggest that the distinction between viral and bacterial meningitis may be potentially difficult in the early stages of disease onset, leading to delayed diagnosis. Therefore, the patient’s condition should be monitored closely and, if necessary, re-examinations should be considered.
Excluding herpes simplex virus infections, most viral meningitis is known to be non-fatal. However, some cases of enterovirus, human herpesvirus 6 infections, and parechovirus [6,24,25] may be accompanied by CSF non-pleocytosis and may cause severe encephalitis, which can be fatal or lead to further complications. Therefore, PCR tests to identify the specific virus that caused meningitis are needed; these tests have the added benefits of reducing the need for further investigations, the number of medications prescribed, and the length of hospital stay.
This study has some limitations. As our work is retrospective in nature, a generalization of the results may not be appropriate. We did not obtain data of CSF examinations in all the included infants. Therefore, further prospective studies are necessary.
In conclusion, we showed that meningitis is not uncommon among infants ≤90 days old who have come to the hospital with a fever. Furthermore, younger age may be negatively correlated with CSF pleocytosis in meningitis. Our results indicate initial CRP levels may not be reliable predictors of bacterial meningitis and that initial leukopenia may be more dependable. Analysis of CSF or inflammatory markers in the peripheral blood is insufficient to diagnose meningitis and to also differentiate between viral and bacterial source, and therefore, PCR tests for various viruses and bacteria may be necessary. Meningitis patients <90 days old have non-specific symptoms and signs and often do not have CSF pleocytosis. It is crucial to closely monitor the patient's condition by analyzing whether the laboratory findings and clinical symptoms are consistent.
Notes
No potential conflict of interest relevant to this article was reported.
Author contribution
Conceptualization: SJY. Data curation: KUC. Formal analysis: KUC. Writing-original draft: KUC. Writing-review & editing: KUC and SJY.
Acknowledgements
We would like to thank Ho Hyeong Jo for his time and useful comments. This work was supported by the 2019 Inje University research grant.