Introduction
Since coronavirus disease 2019 (COVID-19) was declared a global pandemic on March 11, 2020 by the World Health Organization, the COVID-19 pandemic has affected over 373 million people worldwide, of whom approximately 5,678,000 have died and around 295,000,000 have recovered, resulting in significant economic damage [1]. Evidence exists documenting the effects of the COVID-19 pandemic on the psychological and physical welfare of the general population [2]. An online survey of 3,637 COVID-19-free persons from China during the COVID-19 pandemic described increases in the prevalence of insomnia, anxiety, and depressive symptoms [3].
Migraine is one of the most common neurological diseases, for which a genetic predisposition plays a critical role along with internal and external sources of environmental influence, including psychosocial and psycho-emotional challenges, hormonal dysregulation, and dietary factors, among others [4]. Migraine attacks are considered to result from natural fluctuations in neuronal excitability and trigger factors [5]. Stress and post-stress rest are known migraine triggers [6]; Moreover, migraine is associated with various psychiatric comorbidities [7]. For migraine patients, the outbreak of COVID-19 has also had some notable impacts, including negative therapeutic effects and psychological distress [8]. Pediatric migraine is among the most common primary or comorbid neurological disorders in children, with a prevalence ranging from 3% in preschool children to 23% in adolescents [9]. A nationwide survey found that the prevalence of headache among school children was 29.1% in South Korea [10]. Migraine headaches were reported by 8.7% of children (7.0% of boys, 10.3% of girls), tension headaches by 13.7% (10.7% of boys, 16.3% of girls), and others by 6.7%. Pediatric patients with migraine are especially vulnerable to stressful and anxious encounters [4]. Thus, these patients constitute a specific at-risk population that should be monitored for COVID-19-related effects on their headache evolution.
Remarkable negative effects on hospital-based headache care have been reported during the COVID-19 pandemic in studies from Denmark and Norway [11]. A recent study conducted in Italy reported that, during the COVID-19 quarantine, subjects with migraine had fewer migraine attacks and less pain, as well as moderate levels of depression [12]. Although prior studies observed that migraine attack patterns during the COVID-19 pandemic possibly differed from the pre-pandemic patterns [8,12], very limited data have been published on the frequency or severity of migraine attacks in children during the COVID-19 pandemic, except for a cross-sectional study that surveyed migraine frequency [13].
The purpose of this retrospective longitudinal cohort study in children and adolescents with migraine was to compare the frequency and severity of migraine attacks before and during the COVID-19 pandemic, and to identify the potential risk factors for worsening migraine attacks during the pandemic.
Materials and Methods
1. Patient enrollment
We conducted a retrospective longitudinal cohort study involving children and adolescents with migraine between January 2017 and September 2021 at a pediatric neurology clinic affiliated with Pusan National University Children’s Hospital. The inclusion criteria were as follows: (1) age from 6 to 19 years; (2) fully completed headache survey and questionnaire investigating the effect of the COVID-19 pandemic on headache and quality of life; (3) the availability of neuroimaging data to rule out secondary headache with or without significant risk factors; and (4) patients who had been treated for migraine at least 6 months before the COVID-19 pandemic, and who were followed-up with headache diaries and the Pediatric Migraine Disability Assessment (Ped-MIDAS) score for at least 5 months since April 2020. The diagnosis of migraine as a primary headache was made by pediatric headache specialists according to the International Classification of Headache Disorders, third edition [14]. Patients were classified as having migraine with or without aura, chronic migraine, probable migraine, or episodic syndromes associated with migraine. The exclusion criteria were as follows: (1) patients with other types of primary headache; (2) patients with organic brain disease other than migraine; (3) patients with cognitive impairment; (4) administration of other chronic medications for ≥2 months; and (5) patients being treated or previously treated for COVID-19.
2. Clinical evaluation for headache and headache-related disability
Based on medical records and headache diaries, the following information was obtained: duration and frequency of headaches, detailed headache features, accompanying symptoms (nausea/vomiting, dizziness, photophobia, phonophobia, osmophobia, and allodynia), lifestyle factors (sleep cycle, physical activity, school or study work, mood, and stressful situation), and acute and preventive medications for migraine. The questionnaire used in this study is shown in Appendix 1. Patients were asked about the effect of the COVID-19 pandemic on their headaches and quality of life. Patients’ attention and concern about COVID-19 and worsening headaches during the COVID-19 pandemic were evaluated. Significantly worsening headache was defined as occurring if patients described that they had experienced an increase in headache frequency of more than 50% or headache intensity stronger by more than 2 points on average according to the Wong-Baker pain rating scale, compared to their habitual migraine headaches. The total Ped-MIDAS score [15] was used to compare the degree of disability experienced in daily life related to the severity of headache during the 3 months before and after the first declaration of the COVID-19 pandemic in April 2020. The severity of headache was divided into four grades according to the total Ped-MIDAS score (I: little or no disability, 0-5; II: mild disability, 6-10; III: moderate disability, 11-20; IV: severe disability, ≥21). Changes in mood and sleep quality during the COVID-19 pandemic were measured using the 7-point Patient’s Global Impression of Change (PGIC) scale (1, very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; 7, very much worse) [16]. The primary outcomes investigated were as follows: (1) the change in the Ped-MIDAS score during the COVID-19 pandemic, and (2) the predictive risk factors related to aggravation of the Ped-MIDAS score or worsening headache, including sleep, daily activities, mood, and accompanying symptoms.
3. Standard protocol approvals, registrations, and patient consent
This study received ethical approval (number: 05-2022-043) from the Institutional Review Board of Pusan National University Yangsan Hospital. Written informed consent was obtained from each participant and his or her parents or guardians.
4. Statistical analysis
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) using raw scores. To compare patients with and without worsening headache, the two-tailed chi-square or Fisher exact test was used for the analysis of categorical data, and the independent t-test was used for continuous variables with normal distributions. The Mann-Whitney test was used for continuous variables with non-normal distributions. In addition to univariate non-parametric statistical tests, the results of the paired and independent t-tests were confirmed using the Wilcoxon signed-rank test and the Mann-Whitney test. Multiple stepwise linear regression was performed to detect the clinical variables that were predictive of changes in the Ped-MIDAS score before and during the COVID-19 pandemic. Multivariate logistic regression was used to identify independent risk factors related to worsening headaches during the COVID-19 pandemic. Odds ratios with 95% confidence intervals were used to test differences within groups. In all analyses, P values <0.05 were considered to indicate statistical significance. GraphPad Prism for Mac V.8.43 (GraphPad Software, San Diego, CA, USA) was used to generate the figures.
Results
1. Characteristics of migraine patients during the COVID-19 pandemic
Among the 417 initially recruited children and adolescents with migraine, 373 completed the questionnaires and 325 (122 boys and 203 girls) were finally enrolled in this study; 48 patients who were not followed up during the COVID-19 pandemic were excluded (Fig. 1). The mean age of the 325 patients was 12.8±5.6 years (range, 8 to 19), and migraine without aura accounted for the majority (55.1%, 179/325) (Table 1). Nausea/vomiting was the most common accompanying symptom (71.1%), followed by photophobia (62.8%), dizziness (58.5%), phonophobia (52.6%), and osmophobia (47.1%). Acute and preventive treatments for migraine were performed in 97.2% and 59.4% of patients, respectively.
The results of the questionnaire on the effects of COVID-19 on patients' headaches and overall life are summarized in Table 2. The average monthly frequency of migraine headache was 2.17±1.32 before and 4.62±3.29 during the COVID-19 pandemic (P<0.001). Stress increased in 197 (60.6%) patients, and 251 (77.2%) patients reported a decrease in their physical activity. More than 80% of patients reported medium (n=129, 39.7%) to strong (n=145, 44.6%) concerns about COVID-19. The PGIC scores of mood and sleep quality using slightly deteriorated to 4.9 and 4.6 points, respectively. In total, 33.8% of subjects reported increases in acute treatment, and 18.8% described additions to or changes in preventive medication.
2. Changes in and determinants of the Ped-MIDAS score
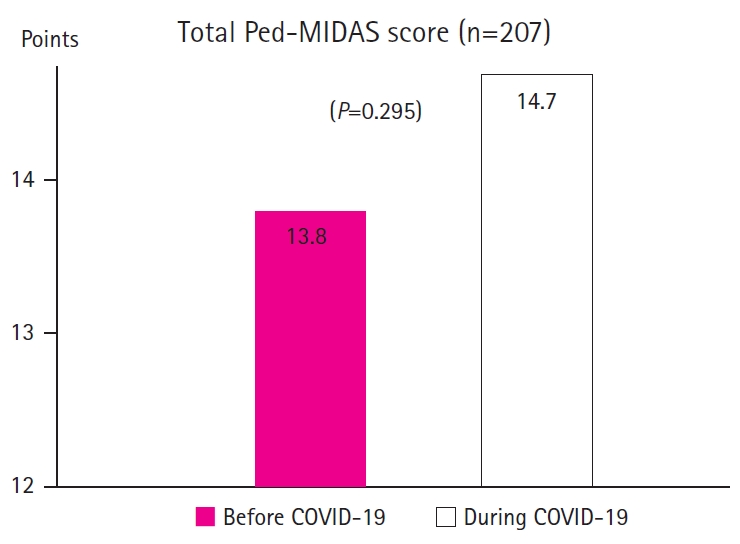
The Ped-MIDAS was administered to 207 patients both before and during the COVID-19 pandemic, and the total score rose slightly from 13.8 (pre-COVID-19) to 14.7 (post-COVID-19) points, but the difference was not statistically significant (P=0.295) (Fig. 2). Multiple regression analysis revealed that younger age (P=0.039), mood deterioration (P<0.001), sleep disturbance (P=0.018), increased acute medication (P=0.011), and worsening headache (P=0.017) were important clinical factors associated with the aggravation of Ped-MIDAS scores during the COVID-19 pandemic (Table 3).
3. Characteristics and risk factors of significantly worsening headache
Sixty (18.5%) of the 325 patients showed significantly worsening migraine headache (Table 4). Patients with worsening headache had significantly higher stress (78.3% vs. 56.6%, P=0.041), were more likely to have strong concerns about COVID-19 (60.0% vs. 41.1%, P=0.032), and their mood (6.1±1.4 vs. 4.1±0.9, P<0.001) and sleep (5.8±1.2 vs. 4.0±0.9, P<0.001) scores were worse than those without worsening headache. An increase in acute treatment (61.7% vs. 27.5%, P<0.001) and an addition or change in preventive therapy (30.0% vs. 16.2%, P=0.025) were significantly more common in patients with worsening headache than in those without. The change in the Ped-MIDAS scores before and during the COVID-19 pandemic (ΔPed-MIDAS=post-COVID-19 Ped-MIDAS minus pre-COVID-19 Ped-MIDAS score) was also significantly higher in patients with worsening headache than in those without (1.9±3.4 vs. 0.5±2.1, P<0.001). Logistic regression analysis showed that younger age (P=0.017), worsening mood (P<0.001), sleep problems (P<0.001), increased acute medication (P=0.010), and a larger ΔPed-MIDAS score (P=0.002) significantly contributed to worsening headache (Table 5).
Discussion
In this study, we evaluated the effects of aspects of individual and social life during the COVID-19 pandemic on migraine headaches and potential risk factors at a single tertiary center. We found that many children and adolescents reported increased stress (60.6%), decreased physical activity (77.2%), moderate or greater concerns about COVID-19 (84.3%), and exacerbated changes in mood and sleep during the COVID-19 pandemic. Moreover, 33.8% reported increased acute treatment for migraine attacks, and 18.8% described additions to or changes in preventive medication. The total Ped-MIDAS score increased (from 13.8% to 14.7%, P=0.295) in 207 patients who had scores available from both before and during the COVID-19 pandemic. Of the 325 patients, 60 (18.5%) had significantly worsening migraine headaches compared to their usual headaches. Multiple logistic regression revealed that younger age, mood deterioration, sleep disturbance, increased acute medication use, and larger changes in Ped-MIDAS scores were potential risk factors for worsening migraine attacks during the COVID-19 pandemic. Other studies have addressed changes in headache days or intensity during the COVID-19 pandemic [13,17], but changes in the total Ped-MIDAS score in children and adolescents with migraine have not been well studied.
In our study, the headache-related disability of all pediatric patients, based on the mean Ped-MIDAS scores, did not significantly increase during the COVID-19 pandemic. This result was contrary to the hypothesis that increased stress negatively impacts headache-related disability in patients with migraine. Recent studies have reported diverse results regarding changes in headache frequency and intensity in migraine patients during the COVID-19 pandemic. In a web survey of 1,018 patients with migraine during the lockdown period, 60% described an increase in migraine frequency, while 16% reported a decrease in migraine frequency. Severe migraine was observed in 64% of patients [13]. In a multicenter cross-sectional study in Japan, the total MIDAS scores of 606 migraine patients did not significantly change after the first wave of the COVID-19 pandemic [18]. Verhagen et al. [17] performed a study in 592 migraine patients and showed that the number of migraine days did not change, the daily use of acute medication decreased, and well-being scores improved after the lockdown during the COVID-19 outbreak. Verhagen et al. [17] suggested that the complex effects of working from home, reductions in demanding social lives, and the relatively comfortable control of one’s working hours contributed to the lack of change in headache conditions during the COVID-19 pandemic. Unlike in the United States and Europe, South Korea conducted a partial closure of public facilities, as opposed to complete shutdowns, during the COVID-19 pandemic. In particular, school management allowed students of different grades to attend school selectively on a weekly basis. Each student took online and offline classes weekly. Compared to high school students, the proportion of online classes in elementary school students was more frequent; frequent online classes resulted in irregular sleep hours and lifestyle patterns, as well as long-time exposure to light stimulation from the screen. Because of these changes in school attendance and class patterns, younger age can be considered as an important risk factor for worsening headache and increases in Ped-MIDAS scores. However, the frequency of online classes was not always proportional to younger age. Even within the same elementary school, the offline class rate was higher in the first and second grades, and it was the highest in the third year of high school. Therefore, interpreting this proposed mechanism purely in terms of age may be erroneous.
Psychological stressors are generally recognized as potential triggers of recurring episodes of pediatric migraine. Stressful and emotionally overwhelming experiences in schools and/or families can contribute to hypersensitivity of the central nervous system, increasing the risk of pediatric migraine attacks [19,20]. Previous studies have reported that adverse life events and stressful events are significantly associated with headache frequency [21,22]. COVID-19 itself is a major social stressful event, and it is already known that a positive correlation exists between major life stress and headache frequency [21]. In our study, we found that 60.6% of patients with pediatric migraines reported increased stress, and patients with worsening headache during the COVID-19 pandemic were more likely to show increased stress than those who did not.
Our study indicated that poor sleep was an independent risk factor for worsening headache and increased Ped-MIDAS scores during the COVID-19 pandemic. Two possibilities can be considered to explain the results based on prior research. First, Schuh-Hofer et al. [23] revealed that migraineurs mobilized 5-hydroxytryptamine from intracellular stores early in a migraine attack. It is noteworthy that 5-hydroxytryptamine plays a diverse role in a variety of human behaviors, including sleep, mood, and pain, and it could promote wakefulness and have a negative effect on sleep [24]. Therefore, poor sleep may be a manifestation of pathways that also lead to frequent migraine attacks. Second, poor sleep may also lower pain thresholds [25]. Previous studies have reported that the relationship between poor sleep and migraine is a series of bidirectional interactions [24]. Fortunately, poor sleep can be modified through medical advice and personal efforts. Therefore, we suggest that it is essential that pediatric neurologists consider evaluating patients’ sleep condition in order to improve their daily life during the COVID-19 period.
Mood disorders are well documented as comorbidities of migraine in children and adolescents [26,27]. Additionally, worsening of migraine attacks was only observed in patients who reported higher anxiety during the COVID-19 lockdown [28]. Anxiety is psychosocial and affective factor involved in pediatric migraine onset and chronicity [26], and similar mechanisms have been theorized to underpin both anxiety and chronic pain [29]. Therefore, children with migraine should be considered as a specific vulnerable population that needs specialized and multi-professional attention during and after the epidemic, as well as during major stressful events.
This study had several limitations. First, this was a retrospective study. Patients were asked to evaluate their condition and fill out questionnaires for the periods 3 to 4 months before and after the declaration of the pandemic. Therefore, this study may have been affected by the recall bias of patients’ self-reports. Second, the assessment of the Ped-MIDAS scores before and during the pandemic was completed in 63.7% of all patients. Third, healthy controls were not included in the study because we focused on changes in clinical symptoms in patients with migraine. Fourth, the PGIC scale was not specifically designed to evaluate mood or sleep changes. Specific anxiety or depression test results for patients with deteriorated mood scores were not included in this study. Fifth, we did not investigate patients' stress, physical activity, mood, and sleep conditions separately before and during the COVID-19 pandemic; instead, we only asked them to describe their changes. Since this study was conducted for 5 months to 1.5 years after the COVID-19 pandemic was declared, the effect of changes in patients' age is thought to be insignificant. Disability of daily life due to headache was compared before and during COVID-19 using Ped-MIDAS scores. Finally, restrictions on school and social activities and the closure of public facilities occurred unexpectedly, and the long-term effects of mental and physical health problems, weight gain, wearing a mask, and changes in lifestyle could not be evaluated.
In conclusion, our results identified that some children and adolescents with migraine during the COVID-19 pandemic suffered from worsening migraine attacks. In addition, several potential risk factors contributing to worsening headache were identified, and it is hoped that the identification of these factors will help manage pediatric migraine patients during the COVID-19 pandemic. We suggested that proactive monitoring of mood swings and sleep disturbance during the COVID-19 pandemic in younger children with migraine can contribute to early identification of the exacerbation of headaches. Future research can be strengthened by adding evaluations that quantify various clinical variables and by expanding the number of patients.